study
TIRED 2
I am so pleased to be able to contact you with the link to the second paper from the TIRED study ‘Need for recovery and physician well-being in Emergency Departments: national survey findings’ paper published in the European Journal of Emergency Medicine.
All contributor names will appear at the end of the article and the article should be able to be accessed through local institutional logins but if you have any issues then please let us know.
Your hard work in sharing and spreading the message of the original TIRED study paper in BMJ Open was brilliant and resulted in the article having an Altmetric of 214, featuring as a 60 second piece in the BMJ in print and is still being picked up with citations and a recent infographic.
So we would encourage you to do the same with this paper and increase the impact on this still very important topic by sharing the paper and results with your colleagues as widely as possible through email and on social media using the hashtag #TIREDSTUDY and feel free to tag in @ternfellow and @lauracottey too. We have attached a document containing the Top 5 outcomes which can be used for social media.
Top tips for increasing engagement with the paper:
- Add the article link to your signature block
-
Share with colleagues that may have taken part by sharing the link/QR code through email, local whatsapp groups and on social media
-
If on platforms like Linkedin or ResearchGate add the paper on there using the DOI
Once again, I cannot thank you all enough for your support of this study and for all the hard work you put in to make it a success. If you have any comments, further requirements or questions please don’t hesitate to contact tern@rcem.ac.uk. TIRED 2!
Laura
The SHED Protocol Is Online!
The SHED Protocol is Online
Study Protocols
Study protocols are a core component of a research studies. They document a study’s rationale, methodology, and planned analyses, and adherence to a protocol is now a part of research legislature (1). These have not always been publicly available, and inconsistencies between protocol and publication have been reported with selective presentation of outcomes (2), inconsistent reporting on methodology (3), and adverse events (4). Trial registries provide a platform for detailing the core components of a study (SHED’s can be found here), but protocols provide additional information beyond what is commonly available on most trial registries (5).
Protocol Publishing
As a result, there has been a move towards publication of study protocols, with entire journals now devoted to the publication of study protocols. Making protocols publicly available informs researchers and participants of upcoming trials and novel research methods, provides greater transparency, and reduces selective publication and reporting of research outcomes, although there is always work to be done (6).
However, there is a problem. Publishing protocols costs money. So how do you adhere to best research practice when you can’t afford it?
As far back as 1999 the internet has been seen as providing a solution to these problems (7). As part of a trend towards greater transparency, the use of preprint publications has grown rapidly over the last twenty years (this wonderful graph tracks the rapid growth in preprints over time). Pre-print publications are presented prior to peer review, with the caveat that it has not been peer-reviewed. During the COVID-19 pandemic the use of preprints increased exponentially as a means of rapidly reporting findings related to this new and novel disease. This image below shows the dramatic rise of preprints.
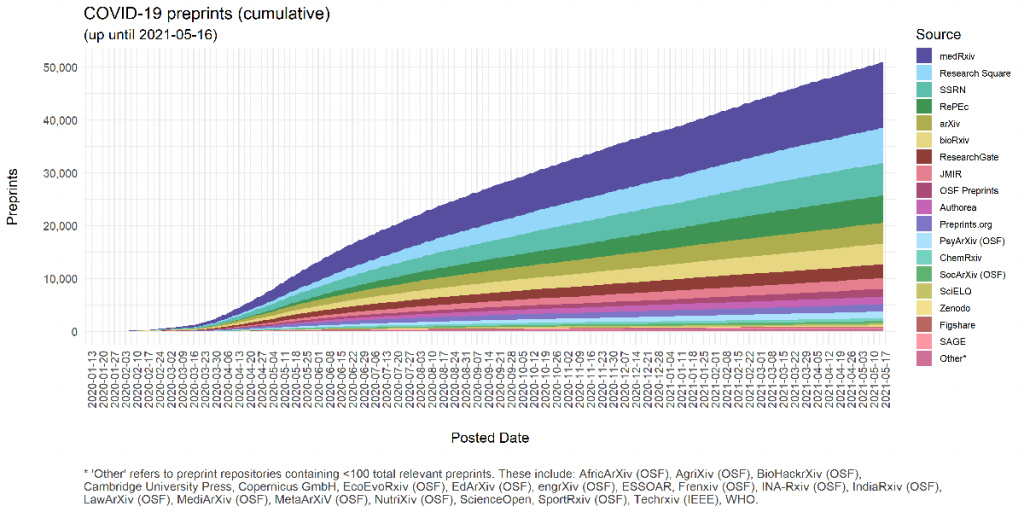
Image courtesy of Nicholas Fraser
{kind=link}
Subarachnoid Haemorrhage in the Emergency Department (SHED)
We are choosing to publish the SHED study protocol as a preprint.
Pre-prints are normally a step towards full publication, a tool to speed up the availability of important research data. However, we are not planning on submitting SHED to a peer-reviewed journal for publication.
We believe that publishing the study protocol is vital for research transparency. Importantly, it will allow our members know more about the study, how it will be run, and get people excited for SHED. It will allow free and open-access to our methodology and ensure that we are held up to the highest research rigor without having to pay for the privilege. We want everyone to be able to read the SHED Protocol.
Despite not submitting for journal peer-review, our study has been reviewed during both the funding and ethical approval process. Indeed, many journals would take these two reviews and accept the protocol for publication – after the open-access payment of course.
Research funding is not infinite, and we have a duty to patients and those sponsoring this study to use the money wisely. We would rather use this limited resource to run the study and increase local research engagement than pay to publish the protocol on a particular journal website rather than a preprint server. Whilst many large studies will not suffer from the thorny dilemma of where best to allocate a limited research budget, many do not have this luxury.
We’re looking forward to running SHED with you all, and getting down to some non-COVID related research. Recruitment will be starting in September / October 2021. Email us here with your questions / comments / suggestions. Tweet about the study and tag us @ternfellow.
References
- European Medicines Agency. International Council for Harmonisation (ICH) E6 – Good Clinical Practice (GCP) (R2) addendum [Internet]. 2016 [cited 2021 Jun 1]. Available from: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e-6-r2-guideline-good-clinical-practice-step-5_en.pdf
- Al-Marzouki S, Roberts I, Evans S, Marshall T. Selective reporting in clinical trials: analysis of trial protocols accepted by The Lancet. The Lancet. 2008 Jul;372(9634):201.
- Chan A-W, Hrobjartsson A, Jorgensen KJ, Gotzsche PC, Altman DG. Discrepancies in sample size calculations and data analyses reported in randomised trials: comparison of publications with protocols. BMJ. 2008 Dec 4;337(dec04 1):a2299–a2299.
- Scharf O, Colevas AD. Adverse Event Reporting in Publications Compared With Sponsor Database for Cancer Clinical Trials. JCO. 2006 Aug 20;24(24):3933–8.
- Skogvoll E, Kramer-Johansen J. Publication of clinical trial protocols – what can we learn? Scand J Trauma Resusc Emerg Med. 2013 Dec;21(1):12, 1757-7241-21–12.
- Cro S, Forbes G, Johnson NA, Kahan BC. Evidence of unexplained discrepancies between planned and conducted statistical analyses: a review of randomised trials. BMC Med. 2020 Dec;18(1):137.
- Chalmers I, Altman DG. How can medical journals help prevent poor medical research? Some opportunities presented by electronic publishing. Lancet. 1999;353(9151):490–3.
CERA 5
CERA 5 is here!
Good evening everyone. The COVID-19 Emergency Responsiveness Assessment study is in its fifth phase. The first three phases looking at the acceleration, peak, and deceleration of the first wave of the COVID-19 pandemic in the UK in 2020. The fourth phase (for which we now have results!) looked at the impact of the third wave. A finding observed in the deceleration phase of the pandemic was a high degree of persisting distress & trauma. Given the impact of the third wave of the pandemic, we are looking to find out how people are feeling, three months after the first survey.
If you completed the first survey, you will have received an invite to this phase of the survey. This phase of the survey - CERA 5 - is open for two weeks. We will then collect the data and send it off to the R-factory. This will allow us to assess the impact of this third wave of the pandemic in the UK, the impact of which persists for many. Our heart goes out to all those affected by the scenes of devastation seen in India.
Hope you're staying safe.
Rob